US health care is, to put it generously, a work in progress. So as we size up its many shortcomings, you might find yourself wondering: Okay, we've got a long to-do list here. Which problem will we tackle first?
Over the past week, I endeavored to find out how some of the sharpest minds in health policy would answer that question. I asked a dozen health care experts what they thought the next big target for health care reform — something that felt genuinely achievable in the next five to 10 years — would be.
We should always remain humble when predicting the future, but it still seems safe to assume a major health care overhaul is not in the cards. (Though Donald Trump is starting to beat the Obamacare repeal drum again, so stay tuned.) Each party governs with a razor-thin margin, and both have been punished electorally the last time they sought to make health care a pillar of their platform (Democrats in 2010 after the Affordable Care Act passed, Republicans in 2018). Barring a dramatic shake-up of American politics, a sweeping reform like Medicare-for-All is not walking through the door.
But that does not mean health policy will not be made.
"Recognizing the hazards of making predictions in politics, I don't see any health reform on the horizon on the scale of the Affordable Care Act," Larry Levitt, executive vice president at the health policy think tank KFF, told me. "But I can imagine various health reforms breaking through, maybe even on a bipartisan basis."
Some of the responses I received about what could come next were obvious, such as closing the Medicaid expansion gap that has left 2 million low-income Americans without health insurance. Others were more surprising, such as the potential for a grand bargain reforming a Medicare program that is quietly being remade already.
But one answer stuck out the most: Almost all of the experts predicted that a segment of the health care sector that has often eluded serious reform efforts in the past could finally find itself a target for policymakers.
Hospital reimbursements
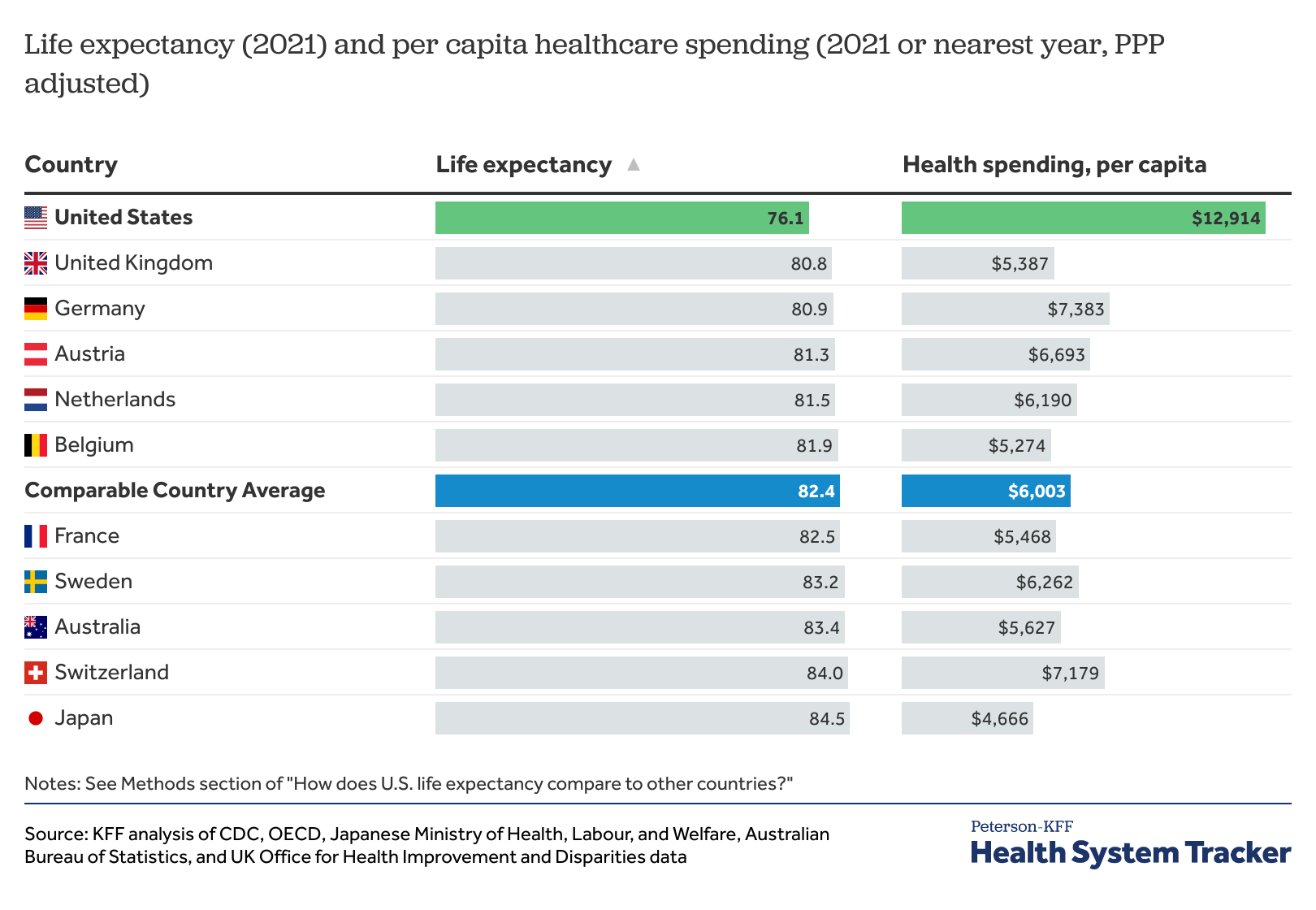
About one out of every three dollars that the US spends on health care goes to hospitals. That alone makes them an obvious target for reform, as US medical spending continues to dramatically outpace its peers.
But hospitals are also a politically potent force. There is a saying around Washington, DC, that every congressional district has a hospital, and that hospital is often one of the largest employers in its community. Threatening its bottom line is inviting the kind of political backlash lawmakers generally try to avoid.
Nevertheless, almost every expert I spoke to cited hospitals as the likely subject of policymaking in the near future. One policy in particular was commonly cited: site-neutral payments.
Under federal law, hospitals can generally charge more for a service performed at one of their outpatient departments than a doctor at a stand-alone practice can charge for the same service. During congressional hearings this year, lawmakers cited studies that found prices at physician practices increased by 14 percent after they were acquired by a hospital.
There is a clear bipartisan interest in correcting what on its face appears to be a transparent perversion in provider payments. Why should the same service cost more just because of where it is performed?
Site-neutral payments would stipulate that Medicare, the largest payer for health care services in the US, would pay the same amount for the same service no matter where it is performed. Blue Cross Blue Shield (consider the source, a health insurer) has estimated site neutrality would save nearly $500 billion over 10 years.
"I do think it's the 'big-ish' policy idea with the most bipartisan appeal at the moment," Matthew Fiedler, a senior fellow with the Brookings Schaeffer Initiative on Health Policy, told me.
In fact, Fiedler told me that he could envision site-neutral payments passing in the near term no matter which party controls Congress and the White House. Democrats could use the expected savings to fund more coverage expansions; in divided government or with the Republicans in charge, cracking down on government payments to hospitals could appeal as a deficit-reduction measure.
Hospitals have said whatever revenue they gain from the current lack of site neutrality is at best a balm because Medicare and Medicaid reimbursements are already too low. And early proposals have sought to ameliorate the effects on hospitals, particularly the ones in a more precarious financial position because they serve more low-income patients.
Other reforms to health law affecting hospitals could include changes in the tax treatment of nonprofit hospitals or stronger requirements for maintaining their nonprofit status as well as alterations to the 340B drug program that provides discounts to hospitals but has become a heated point of contention between hospitals and the pharmaceutical sector.
But site-neutral payments look like the best bet as of now.
"Site-neutral payment seems like it will happen," Katherine Hempstead, a senior policy adviser at the Robert Wood Johnson Foundation, told me.
Health insurance expansion
The US has edged closer to universal health care since the Affordable Care Act passed: More than 90 percent of Americans now have some kind of health coverage.
But two problems remain: One, there are nearly 30 million people who are still uninsured. Two, many of the people who do technically have health insurance still struggle to afford their out-of-pocket obligations under their insurance plan. That made the continued expansion of insurance benefits another commonly cited subject for near-term reforms.
One of the most obvious policy actions would be permanently extending the enhanced federal assistance that was put in place as part of the Inflation Reduction Act, which made more people eligible for ACA subsidies and made those subsidies more generous for the people who already qualify. The enhanced subsidies are scheduled to expire in two years but, if Democrats control Congress, "it is very likely" they will be extended, Fiedler said. Even if there is a split government, he said, it's possible the marketplace subsidies could be extended as part of a larger tax deal between the two parties.
If Democrats can wrestle back full control of the government, experts also expect them to finally find a solution to the ACA's Medicaid expansion gap. To recap: Medicaid expansion was supposed to be mandatory for every state, covering all Americans in or near poverty. But the Supreme Court ruled in 2012 that states must have a choice about whether or not to participate in the expansion, which 10 states have still not adopted. That has left 2 million people without any affordable insurance options, many of them people of color living in the South.
Congress could work around those states, covering those people through a federal program or providing more generous financial incentives for states to finally join up. Either way, closing the coverage gap would go a long way toward fully realizing the vision of the ACA when it first passed and, as a result, covering millions more marginalized people who have been left out of the law's gains.
"Filling in the Medicaid coverage gap, in particular, would be a pretty big deal," Loren Adler, associate director at the Brookings Schaeffer Initiative on Health Policy, said.
Permanent solutions to those structural flaws in the ACA (the former lack of marketplace subsidies for people above a certain income and the Medicaid expansion) would be the low-hanging fruit for expanding coverage and making health care more affordable. But if Congress were to get more ambitious, Levitt said, addressing affordability for the employer plans that cover half of Americans would be the next step.
"The Affordable Care Act did a tremendous amount to expand coverage," he said. "But it did little to make health care more affordable for the large number of people who get insurance through an employer."
Then again, Donald Trump has been on the campaign trail reviving his failed plans for repealing the ACA. That would mean dramatic cuts to Medicaid and the possibility of instituting Medicaid work requirements as Republicans have repeatedly agitated for, as well as fierce fights over the continued existence of federal assistance for private coverage and the law's regulations protecting people with preexisting conditions.
Depending on how the politics shake out, the ACA could either be made stronger than it's ever been or its defenders could be left fighting to save it from extinction. It is a reminder of how uncertain the future of any policymaking can be.
Some kind of grand bargain on Medicare
One recurring answer surprised me more than most: the possibility of some kind of grand bargain on Medicare.
But there is a good reason the nation's largest (by spending) insurance program kept coming up in these conversations. Actually, there are two. First, the program's hospital insurance trust fund is projected to run out within the next 10 years, putting pressure on lawmakers to find ways to make it more financially sustainable in the long run. Second, as more and more people flock to privately administered Medicare Advantage plans instead of the traditional government program, lawmakers might want to try to better balance the two.
"The other major health reform I could see, and which might be possible under different political configurations, is a Medicare reform package focused on leveling the playing field between traditional Medicare and Medicare Advantage," Adler said.
Patients are increasingly opting for Medicare Advantage because it's simpler (patients have only one insurance card instead of potentially three under traditional Medicare + Part D + a supplement plan) and because its benefits are more comprehensive (many MA plans cover dental, vision, and hearing, benefits excluded from the traditional program).
Lawmakers could add those critical benefits to traditional Medicare. Adler outlined a package that could include out-of-pocket maximums in traditional Medicare and more restrictions on supplemental coverage. Congress could also address the "benchmarks" that are used to determine how much Medicare Advantage plans are paid, in an effort to find more savings. At the same time, they could grant MA plans more flexibility about how they administer the program's benefits.
Both parties could stand to win: Democrats by strengthening the traditional program and Republicans by getting additional flexibility for Medicare Advantage and, possibly, less federal spending.
The odds are probably against it: Both parties love to attack the other over proposed alterations to Medicare, whether real or imagined. But some kind of Medicare compromise was named by several experts I spoke to as a possible action item in the coming years.
"Certainly a bit of a long shot," Adler said. "Just less of a long shot than any other big bipartisan change I could see."
In US health policy, the best bet is that the status quo will prevail. But if you're wondering what might happen next, these policies are a good place to start.